
Credentialing for Telehealth in 2026: State Rules, Cross-State Practice, and What Most Practices Get Wrong
Telehealth continues to transform healthcare in 2026 — but delivering virtual care across state lines remains a regulatory challenge. Despite rapid adoption, state licensing laws did not become more flexible. In fact, many states have become stricter about verifying licensure, enforcing supervision requirements, and requiring telehealth-specific registration.
This guide breaks down what healthcare organizations need to know to stay compliant and avoid costly mistakes.

Why Telehealth Licensing Still Matters in 2026
Even though telehealth has become mainstream, the legal rule remains unchanged:
Providers must be licensed in the state where the patient is physically located during the visit.
This makes cross-state care complex for physicians, NPs, PAs, and therapists — especially as multi-state telehealth networks continue to expand.
Reference:
U.S. Department of Health & Human Services – Licensing Across State Lines
https://telehealth.hhs.gov/licensure/licensing-across-state-lines
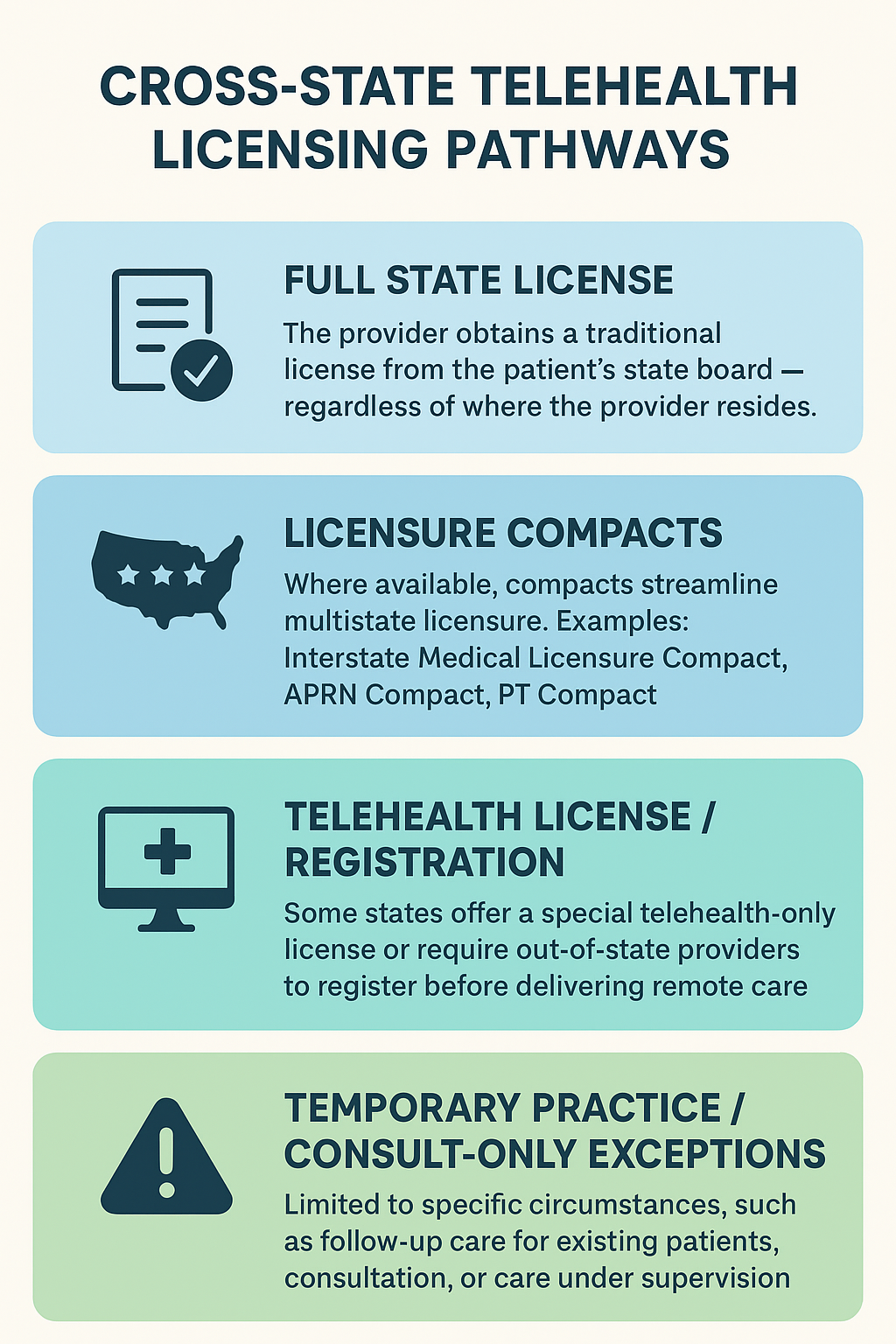
Cross-State Telehealth Licensing Pathways
Understanding how providers can legally deliver telehealth across state lines is essential for 2026 compliance. Below is a visual breakdown of the four primary licensing pathways used by medical groups, hospitals, and telehealth organizations. Each option comes with different requirements, limitations, and administrative workloads.
This table outlines the four major licensure routes providers can use when treating patients across state lines.
To learn more about each category:
https://telehealth.hhs.gov/licensure/licensure-compacts
https://www.cchpca.org
Licensure Compacts & What They Do (and Don’t) Solve
Compacts help significantly — but they are not national licenses. Providers still must obtain a valid license (or privilege to practice) for each state.
Key Compacts Affecting Telehealth in 2026
IMLC (Interstate Medical Licensure Compact) – Physicians
NLC (Nurse Licensure Compact) – RNs & LPNs
APRN Compact – Advanced Practice Registered Nurses
PT Compact – Physical Therapists
ASLP-IC – Audiology & Speech-Language Pathology
Compact map & updates:
https://www.imlcc.org
https://ncsbn.org/nurse-licensure-compact
https://ptcompact.org
Common Misconception
“Joining a compact gives a national license.”
❌ Incorrect.
It gives faster access to state licenses, not one universal license.
The Most Common Compliance Mistakes Telehealth Practices Make
1. Assuming pandemic-era waivers still apply
Nearly all emergency telehealth licensure waivers have expired.
State waiver tracker:
https://www.hopkinsmedicine.org/telemedicine/state-changes
2. Not tracking the patient’s location during visits
The patient’s physical location determines the required license — not their home address.
3. Missing telehealth-specific state registrations
States like Florida, Arizona, and Colorado require telehealth registration before remote care is allowed.
Full state-by-state breakdown:
https://www.cchpca.org/resources
4. Confusing “compact eligibility” with “compact participation”
Some states have passed compact legislation but have not fully implemented it yet. What’s the difference: “Compact eligibility” vs. “Compact participation”
Compact participation means a state has formally adopted the compact via legislation (and the compact is in effect in that state). Only in participating states can a provider get a license through the compact pathway.
Compact eligibility refers to whether a provider meets the criteria (e.g. holds an unrestricted license in a participating state, meets training and background-check requirements) so they can access the compact.
Confusing the two is a common mistake — some assume that because a provider is “eligible,” they can automatically practice across all states, even if a target state hasn’t joined the compact. But that’s incorrect — the target/patient-state still must be a “participating state.”
Examples: Current State Participation in Major Compacts (as of 2025)
Interstate Medical Licensure Compact (IMLC) — for physicians (MD/DO)
As of late 2025, IMLC includes ≈ 42 U.S. states + District of Columbia + Guam.
Participating States
Alabama, Arizona, Colorado, Delaware, Florida, Georgia, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Maryland, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Jersey, North Dakota, Ohio, Oklahoma, Pennsylvania, South Dakota, Tennessee, Texas, Utah, Vermont, Washington, West Virginia, Wisconsin, Wyoming — among others.
States that recently joined or have pending implementation (as of 2025): e.g. Arkansas, North Carolina.
Non-participating (non-member) states / territories:
Alaska
California
Oregon
South Carolina
Virginia
Puerto Rico (territory)
U.S. Virgin Islands (territory)
Advanced Practice Registered Nurse Compact (APRN Compact) — for advanced practice nurses (NPs, CRNAs, etc.)
As of early 2025, only four states had fully enacted the APRN Compact and are active members:
Delaware
North Dakota
South Dakota
Utah
That means even if a nurse meets “compact eligibility,” they can only use the compact if both their home state and the patient’s state are among these four (or other future adopting states).
Why This Confusion (Eligibility vs Participation) Matters — Especially for Telehealth & Multi-State Credentialing
If a provider assumes compact membership — but the state where the patient is located hasn’t adopted the compact — they may be practicing without a valid state license.
For credentialing teams: assuming compact privilege translates to national coverage can lead to compliance issues, licensing denials, or even liability.
For telehealth expansion: it's critical to track not just your providers’ home-state licenses, but the compact status of each patient state before launching cross-state care.
5. Ignoring prescribing rules
Many states restrict prescribing controlled substances through telehealth without an in-person exam.
6. Missing renewal deadlines across multiple states
Telehealth groups with 20+ states can easily fall out of compliance without centralized tracking.
How Healthcare Groups Can Stay Compliant in 2026
1. Maintain a real-time licensing roster
Track every provider’s license, renewal, compact status, and telehealth registration.
2. Confirm patient location at every telehealth visit
Platforms should log the patient’s physical location for compliance documentation.
3. Use licensure compacts strategically
Physicians, nurses, and PTs can onboard much faster using compact privileges.
4. Assign a compliance or credentialing lead
Telehealth compliance is too complex to “split between admins.” It requires an expert.
5. Adopt continuous license monitoring
Monthly or automated monitoring is becoming standard for multi-state operations.
6. Partner with a credentialing firm if scaling nationally
Organizations expanding to 10, 20, or 50 states benefit from outsourcing licensing and credentialing to specialists.
Conclusion
Telehealth is here to stay — but cross-state licensure is more complex than ever. The organizations succeeding in 2026 are the ones investing in strong credentialing systems, leveraging licensure compacts, and maintaining airtight compliance workflows.
With the right processes, telehealth providers can deliver safe, compliant care to patients anywhere in the United States.